 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeCasey C. Bennett
Artificial Intelligence for Diabetes Case Management: The Intersection of Physical and Mental Health
Oct 06, 2018
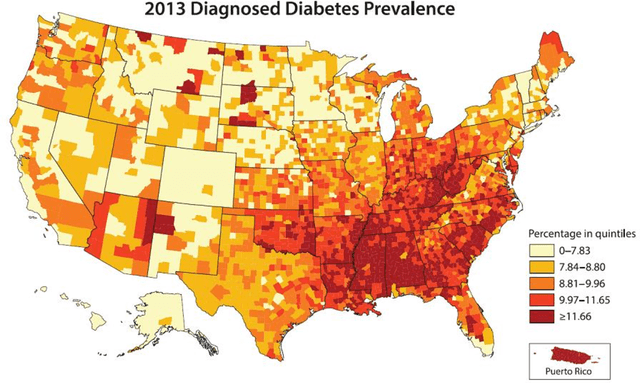
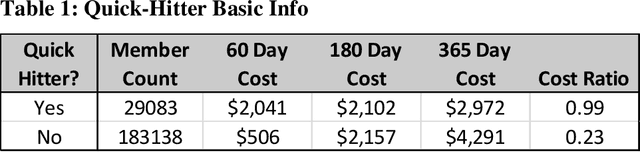

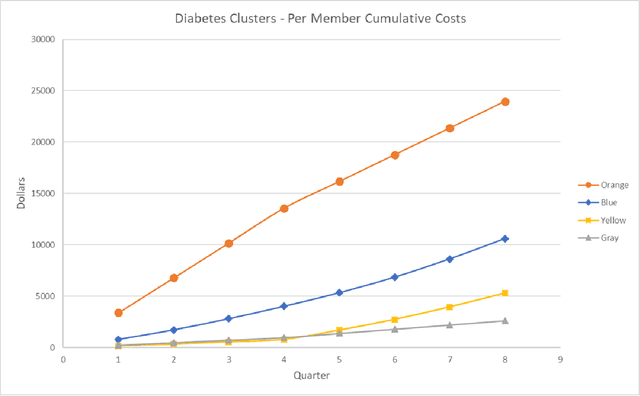
Diabetes is a major public health problem in the United States, affecting roughly 30 million people. Diabetes complications, along with the mental health comorbidities that often co-occur with them, are major drivers of high healthcare costs, poor outcomes, and reduced treatment adherence in diabetes. Here, we evaluate in a large state-wide population whether we can use artificial intelligence (AI) techniques to identify clusters of patient trajectories within the broader diabetes population in order to create cost-effective, narrowly-focused case management intervention strategies to reduce development of complications. This approach combined data from: 1) claims, 2) case management notes, and 3) social determinants of health from ~300,000 real patients between 2014 and 2016. We categorized complications as five types: Cardiovascular, Neuropathy, Opthalmic, Renal, and Other. Modeling was performed combining a variety of machine learning algorithms, including supervised classification, unsupervised clustering, natural language processing of unstructured care notes, and feature engineering. The results showed that we can predict development of diabetes complications roughly 83.5% of the time using claims data or social determinants of health data. They also showed we can reveal meaningful clusters in the patient population related to complications and mental health that can be used to cost-effective screening program, reducing the number of patients to be screened down by 85%. This study outlines creation of an AI framework to develop protocols to better address mental health comorbidities that lead to complications development in the diabetes population. Future work is described that outlines potential lines of research and the need for better addressing the 'people side' of the equation.
Artificial Intelligence Framework for Simulating Clinical Decision-Making: A Markov Decision Process Approach
Jan 10, 2013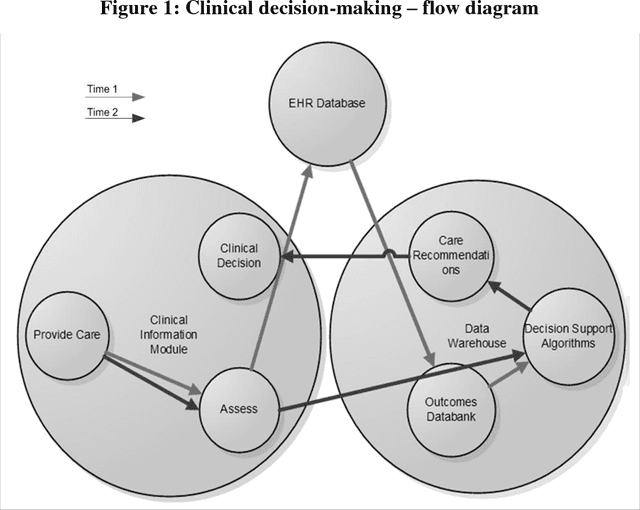
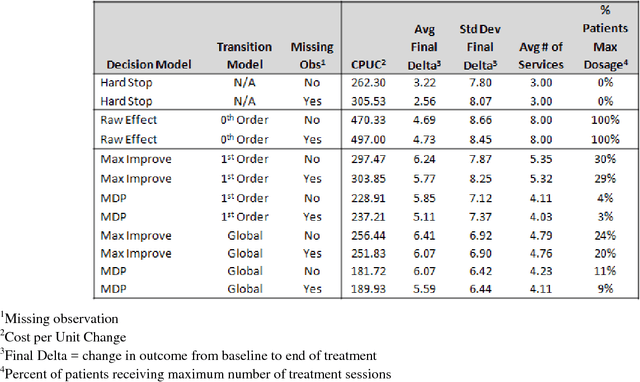
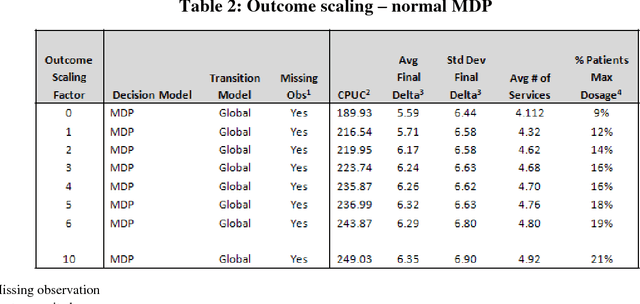
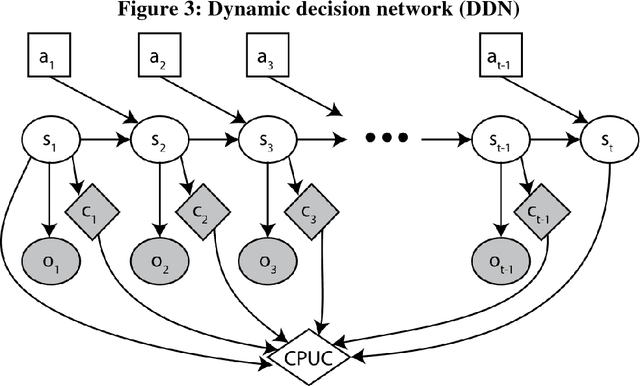
In the modern healthcare system, rapidly expanding costs/complexity, the growing myriad of treatment options, and exploding information streams that often do not effectively reach the front lines hinder the ability to choose optimal treatment decisions over time. The goal in this paper is to develop a general purpose (non-disease-specific) computational/artificial intelligence (AI) framework to address these challenges. This serves two potential functions: 1) a simulation environment for exploring various healthcare policies, payment methodologies, etc., and 2) the basis for clinical artificial intelligence - an AI that can think like a doctor. This approach combines Markov decision processes and dynamic decision networks to learn from clinical data and develop complex plans via simulation of alternative sequential decision paths while capturing the sometimes conflicting, sometimes synergistic interactions of various components in the healthcare system. It can operate in partially observable environments (in the case of missing observations or data) by maintaining belief states about patient health status and functions as an online agent that plans and re-plans. This framework was evaluated using real patient data from an electronic health record. Such an AI framework easily outperforms the current treatment-as-usual (TAU) case-rate/fee-for-service models of healthcare (Cost per Unit Change: $189 vs. $497) while obtaining a 30-35% increase in patient outcomes. Tweaking certain model parameters further enhances this advantage, obtaining roughly 50% more improvement for roughly half the costs. Given careful design and problem formulation, an AI simulation framework can approximate optimal decisions even in complex and uncertain environments. Future work is described that outlines potential lines of research and integration of machine learning algorithms for personalized medicine.
* Keywords: Markov Decision Process; Dynamic Decision Network; Multi-Agent System; Clinical Artificial Intelligence; Medical Decision Making; Chronic Illness; (2013) Artificial Intelligence in Medicine