 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeOliver Speck
PULASki: Learning inter-rater variability using statistical distances to improve probabilistic segmentation
Dec 25, 2023
In the domain of medical imaging, many supervised learning based methods for segmentation face several challenges such as high variability in annotations from multiple experts, paucity of labelled data and class imbalanced datasets. These issues may result in segmentations that lack the requisite precision for clinical analysis and can be misleadingly overconfident without associated uncertainty quantification. We propose the PULASki for biomedical image segmentation that accurately captures variability in expert annotations, even in small datasets. Our approach makes use of an improved loss function based on statistical distances in a conditional variational autoencoder structure (Probabilistic UNet), which improves learning of the conditional decoder compared to the standard cross-entropy particularly in class imbalanced problems. We analyse our method for two structurally different segmentation tasks (intracranial vessel and multiple sclerosis (MS) lesion) and compare our results to four well-established baselines in terms of quantitative metrics and qualitative output. Empirical results demonstrate the PULASKi method outperforms all baselines at the 5\% significance level. The generated segmentations are shown to be much more anatomically plausible than in the 2D case, particularly for the vessel task. Our method can also be applied to a wide range of multi-label segmentation tasks and and is useful for downstream tasks such as hemodynamic modelling (computational fluid dynamics and data assimilation), clinical decision making, and treatment planning.
MedShapeNet -- A Large-Scale Dataset of 3D Medical Shapes for Computer Vision
Sep 12, 2023
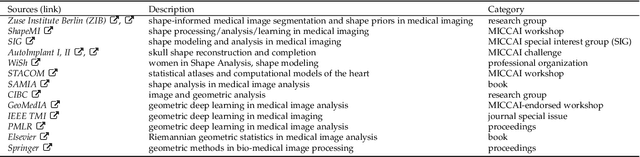

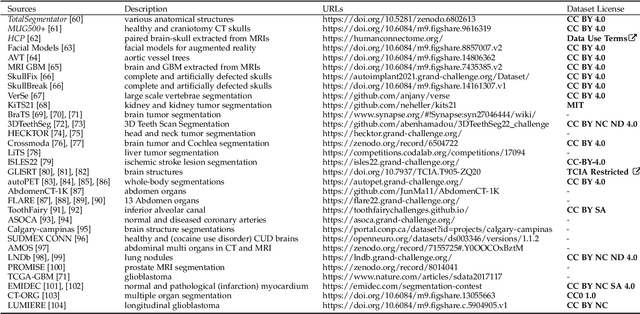
We present MedShapeNet, a large collection of anatomical shapes (e.g., bones, organs, vessels) and 3D surgical instrument models. Prior to the deep learning era, the broad application of statistical shape models (SSMs) in medical image analysis is evidence that shapes have been commonly used to describe medical data. Nowadays, however, state-of-the-art (SOTA) deep learning algorithms in medical imaging are predominantly voxel-based. In computer vision, on the contrary, shapes (including, voxel occupancy grids, meshes, point clouds and implicit surface models) are preferred data representations in 3D, as seen from the numerous shape-related publications in premier vision conferences, such as the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), as well as the increasing popularity of ShapeNet (about 51,300 models) and Princeton ModelNet (127,915 models) in computer vision research. MedShapeNet is created as an alternative to these commonly used shape benchmarks to facilitate the translation of data-driven vision algorithms to medical applications, and it extends the opportunities to adapt SOTA vision algorithms to solve critical medical problems. Besides, the majority of the medical shapes in MedShapeNet are modeled directly on the imaging data of real patients, and therefore it complements well existing shape benchmarks comprising of computer-aided design (CAD) models. MedShapeNet currently includes more than 100,000 medical shapes, and provides annotations in the form of paired data. It is therefore also a freely available repository of 3D models for extended reality (virtual reality - VR, augmented reality - AR, mixed reality - MR) and medical 3D printing. This white paper describes in detail the motivations behind MedShapeNet, the shape acquisition procedures, the use cases, as well as the usage of the online shape search portal: https://medshapenet.ikim.nrw/
Liver Segmentation in Time-resolved C-arm CT Volumes Reconstructed from Dynamic Perfusion Scans using Time Separation Technique
Feb 09, 2023



Perfusion imaging is a valuable tool for diagnosing and treatment planning for liver tumours. The time separation technique (TST) has been successfully used for modelling C-arm cone-beam computed tomography (CBCT) perfusion data. The reconstruction can be accompanied by the segmentation of the liver - for better visualisation and for generating comprehensive perfusion maps. Recently introduced Turbolift learning has been seen to perform well while working with TST reconstructions, but has not been explored for the time-resolved volumes (TRV) estimated out of TST reconstructions. The segmentation of the TRVs can be useful for tracking the movement of the liver over time. This research explores this possibility by training the multi-scale attention UNet of Turbolift learning at its third stage on the TRVs and shows the robustness of Turbolift learning since it can even work efficiently with the TRVs, resulting in a Dice score of 0.864$\pm$0.004.
Complex Network for Complex Problems: A comparative study of CNN and Complex-valued CNN
Feb 09, 2023



Neural networks, especially convolutional neural networks (CNN), are one of the most common tools these days used in computer vision. Most of these networks work with real-valued data using real-valued features. Complex-valued convolutional neural networks (CV-CNN) can preserve the algebraic structure of complex-valued input data and have the potential to learn more complex relationships between the input and the ground-truth. Although some comparisons of CNNs and CV-CNNs for different tasks have been performed in the past, a large-scale investigation comparing different models operating on different tasks has not been conducted. Furthermore, because complex features contain both real and imaginary components, CV-CNNs have double the number of trainable parameters as real-valued CNNs in terms of the actual number of trainable parameters. Whether or not the improvements in performance with CV-CNN observed in the past have been because of the complex features or just because of having double the number of trainable parameters has not yet been explored. This paper presents a comparative study of CNN, CNNx2 (CNN with double the number of trainable parameters as the CNN), and CV-CNN. The experiments were performed using seven models for two different tasks - brain tumour classification and segmentation in brain MRIs. The results have revealed that the CV-CNN models outperformed the CNN and CNNx2 models.
Liver Segmentation using Turbolift Learning for CT and Cone-beam C-arm Perfusion Imaging
Jul 20, 2022



Model-based reconstruction employing the time separation technique (TST) was found to improve dynamic perfusion imaging of the liver using C-arm cone-beam computed tomography (CBCT). To apply TST using prior knowledge extracted from CT perfusion data, the liver should be accurately segmented from the CT scans. Reconstructions of primary and model-based CBCT data need to be segmented for proper visualisation and interpretation of perfusion maps. This research proposes Turbolift learning, which trains a modified version of the multi-scale Attention UNet on different liver segmentation tasks serially, following the order of the trainings CT, CBCT, CBCT TST - making the previous trainings act as pre-training stages for the subsequent ones - addressing the problem of limited number of datasets for training. For the final task of liver segmentation from CBCT TST, the proposed method achieved an overall Dice scores of 0.874$\pm$0.031 and 0.905$\pm$0.007 in 6-fold and 4-fold cross-validation experiments, respectively - securing statistically significant improvements over the model, which was trained only for that task. Experiments revealed that Turbolift not only improves the overall performance of the model but also makes it robust against artefacts originating from the embolisation materials and truncation artefacts. Additionally, in-depth analyses confirmed the order of the segmentation tasks. This paper shows the potential of segmenting the liver from CT, CBCT, and CBCT TST, learning from the available limited training data, which can possibly be used in the future for the visualisation and evaluation of the perfusion maps for the treatment evaluation of liver diseases.
Automated SSIM Regression for Detection and Quantification of Motion Artefacts in Brain MR Images
Jun 14, 2022



Motion artefacts in magnetic resonance brain images are a crucial issue. The assessment of MR image quality is fundamental before proceeding with the clinical diagnosis. If the motion artefacts alter a correct delineation of structure and substructures of the brain, lesions, tumours and so on, the patients need to be re-scanned. Otherwise, neuro-radiologists could report an inaccurate or incorrect diagnosis. The first step right after scanning a patient is the "\textit{image quality assessment}" in order to decide if the acquired images are diagnostically acceptable. An automated image quality assessment based on the structural similarity index (SSIM) regression through a residual neural network has been proposed here, with the possibility to perform also the classification in different groups - by subdividing with SSIM ranges. This method predicts SSIM values of an input image in the absence of a reference ground truth image. The networks were able to detect motion artefacts, and the best performance for the regression and classification task has always been achieved with ResNet-18 with contrast augmentation. Mean and standard deviation of residuals' distribution were $\mu=-0.0009$ and $\sigma=0.0139$, respectively. Whilst for the classification task in 3, 5 and 10 classes, the best accuracies were 97, 95 and 89\%, respectively. The obtained results show that the proposed method could be a tool in supporting neuro-radiologists and radiographers in evaluating the image quality before the diagnosis.
Weakly-supervised segmentation using inherently-explainable classification models and their application to brain tumour classification
Jun 10, 2022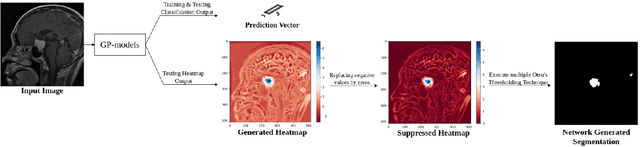
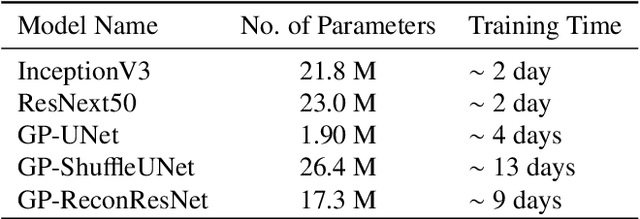
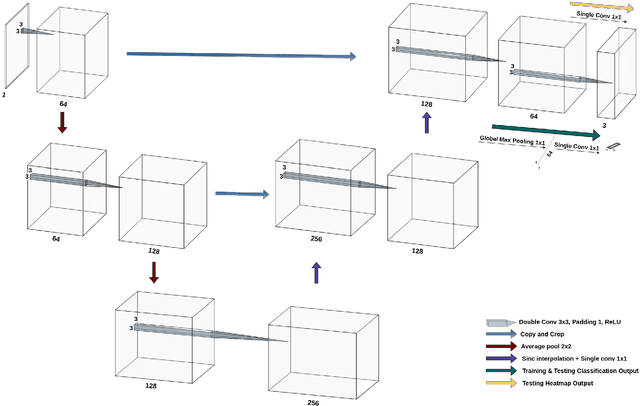
Deep learning models have shown their potential for several applications. However, most of the models are opaque and difficult to trust due to their complex reasoning - commonly known as the black-box problem. Some fields, such as medicine, require a high degree of transparency to accept and adopt such technologies. Consequently, creating explainable/interpretable models or applying post-hoc methods on classifiers to build trust in deep learning models are required. Moreover, deep learning methods can be used for segmentation tasks, which typically require hard-to-obtain, time-consuming manually-annotated segmentation labels for training. This paper introduces three inherently-explainable classifiers to tackle both of these problems as one. The localisation heatmaps provided by the networks -- representing the models' focus areas and being used in classification decision-making -- can be directly interpreted, without requiring any post-hoc methods to derive information for model explanation. The models are trained by using the input image and only the classification labels as ground-truth in a supervised fashion - without using any information about the location of the region of interest (i.e. the segmentation labels), making the segmentation training of the models weakly-supervised through classification labels. The final segmentation is obtained by thresholding these heatmaps. The models were employed for the task of multi-class brain tumour classification using two different datasets, resulting in the best F1-score of 0.93 for the supervised classification task while securing a median Dice score of 0.67$\pm$0.08 for the weakly-supervised segmentation task. Furthermore, the obtained accuracy on a subset of tumour-only images outperformed the state-of-the-art glioma tumour grading binary classifiers with the best model achieving 98.7\% accuracy.
MICDIR: Multi-scale Inverse-consistent Deformable Image Registration using UNetMSS with Self-Constructing Graph Latent
Mar 08, 2022



Image registration is the process of bringing different images into a common coordinate system - a technique widely used in various applications of computer vision, such as remote sensing, image retrieval, and most commonly in medical imaging. Deep Learning based techniques have been applied successfully to tackle various complex medical image processing problems, including medical image registration. Over the years, several image registration techniques have been proposed using deep learning. Deformable image registration techniques such as Voxelmorph have been successful in capturing finer changes and providing smoother deformations. However, Voxelmorph, as well as ICNet and FIRE, do not explicitly encode global dependencies (i.e. the overall anatomical view of the supplied image) and therefore can not track large deformations. In order to tackle the aforementioned problems, this paper extends the Voxelmorph approach in three different ways. To improve the performance in case of small as well as large deformations, supervision of the model at different resolutions have been integrated using a multi-scale UNet. To support the network to learn and encode the minute structural co-relations of the given image-pairs, a self-constructing graph network (SCGNet) has been used as the latent of the multi-scale UNet - which can improve the learning process of the model and help the model to generalise better. And finally, to make the deformations inverse-consistent, cycle consistency loss has been employed. On the task of registration of brain MRIs, the proposed method achieved significant improvements over ANTs and VoxelMorph, obtaining a Dice score of 0.8013$\pm$0.0243 for intramodal and 0.6211$\pm$0.0309 for intermodal, while VoxelMorph achieved 0.7747$\pm$0.0260 and 0.6071$\pm$0.0510, respectively.
DDoS-UNet: Incorporating temporal information using Dynamic Dual-channel UNet for enhancing super-resolution of dynamic MRI
Feb 10, 2022



Magnetic resonance imaging (MRI) provides high spatial resolution and excellent soft-tissue contrast without using harmful ionising radiation. Dynamic MRI is an essential tool for interventions to visualise movements or changes of the target organ. However, such MRI acquisition with high temporal resolution suffers from limited spatial resolution - also known as the spatio-temporal trade-off of dynamic MRI. Several approaches, including deep learning based super-resolution approaches, have been proposed to mitigate this trade-off. Nevertheless, such an approach typically aims to super-resolve each time-point separately, treating them as individual volumes. This research addresses the problem by creating a deep learning model which attempts to learn both spatial and temporal relationships. A modified 3D UNet model, DDoS-UNet, is proposed - which takes the low-resolution volume of the current time-point along with a prior image volume. Initially, the network is supplied with a static high-resolution planning scan as the prior image along with the low-resolution input to super-resolve the first time-point. Then it continues step-wise by using the super-resolved time-points as the prior image while super-resolving the subsequent time-points. The model performance was tested with 3D dynamic data that was undersampled to different in-plane levels. The proposed network achieved an average SSIM value of 0.951$\pm$0.017 while reconstructing the lowest resolution data (i.e. only 4\% of the k-space acquired) - which could result in a theoretical acceleration factor of 25. The proposed approach can be used to reduce the required scan-time while achieving high spatial resolution.
StRegA: Unsupervised Anomaly Detection in Brain MRIs using a Compact Context-encoding Variational Autoencoder
Jan 31, 2022



Expert interpretation of anatomical images of the human brain is the central part of neuro-radiology. Several machine learning-based techniques have been proposed to assist in the analysis process. However, the ML models typically need to be trained to perform a specific task, e.g., brain tumour segmentation or classification. Not only do the corresponding training data require laborious manual annotations, but a wide variety of abnormalities can be present in a human brain MRI - even more than one simultaneously, which renders representation of all possible anomalies very challenging. Hence, a possible solution is an unsupervised anomaly detection (UAD) system that can learn a data distribution from an unlabelled dataset of healthy subjects and then be applied to detect out of distribution samples. Such a technique can then be used to detect anomalies - lesions or abnormalities, for example, brain tumours, without explicitly training the model for that specific pathology. Several Variational Autoencoder (VAE) based techniques have been proposed in the past for this task. Even though they perform very well on controlled artificially simulated anomalies, many of them perform poorly while detecting anomalies in clinical data. This research proposes a compact version of the "context-encoding" VAE (ceVAE) model, combined with pre and post-processing steps, creating a UAD pipeline (StRegA), which is more robust on clinical data, and shows its applicability in detecting anomalies such as tumours in brain MRIs. The proposed pipeline achieved a Dice score of 0.642$\pm$0.101 while detecting tumours in T2w images of the BraTS dataset and 0.859$\pm$0.112 while detecting artificially induced anomalies, while the best performing baseline achieved 0.522$\pm$0.135 and 0.783$\pm$0.111, respectively.